

PCOS - how Permanence can help
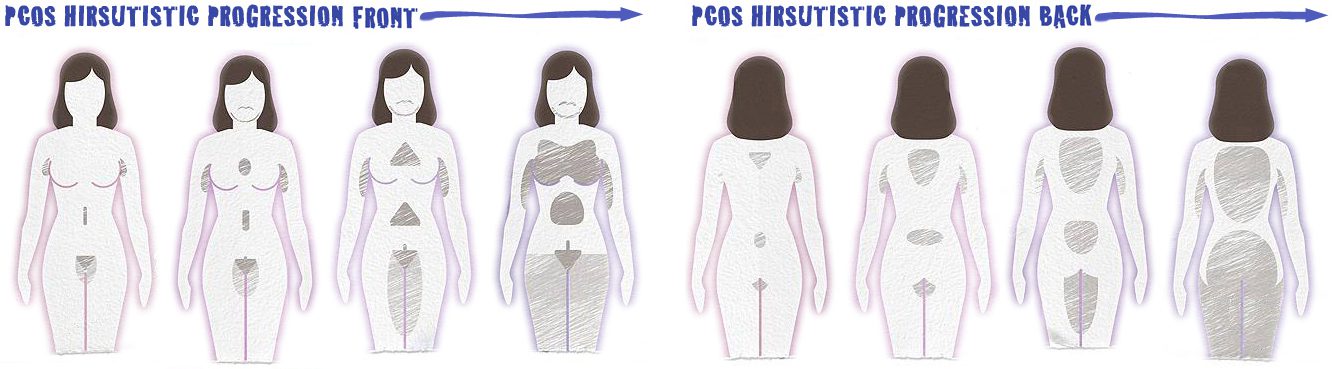
PCOS induced hormone imbalances causing Hirsutism (male pattern hair growth in a female) can be treated, however the growth of darker hair never goes away. At Permanence, we are experts in our field, and using our unique galvanic multi-probe electrolysis method, we treat each individual follicle of unwanted hair with precision accuracy and offer the best results in hair removal for women with PCOS, regardless of where the hair grows, your age, or ethnicity. We understand how important having the freedom of unwanted hair removed is.
At birth our bodies are covered in vellus hair (fine down-like hair) even on our heads but our skin already has all of the hair follicles it will ever have – some 5 million of them. At puberty, androgenic hair growth will cause areas of this vellus hair to convert to terminal hair (thick, long, pigmented hair) on our underarms and pubic region. In males, hormones will also cause terminal hair to grow on the face, chest and, to a lesser degree, on the arms, legs, and back.
In women, the remaining vellus hair can be triggered by hormones to terminal conversion and, once triggered, can’t be reversed.
The only permanent solution to unwanted terminal hair is to kill the hair follicle. Plucking, waxing and laser can only remove the hair stem and, in the case of laser, do some damage to the bulb from which it grows. In each case the hair will recover and grow back.
Our refined galvanic multi-probe electrolysis method treats each individual follicle of unwanted hair with precision accuracy. It’s why we back our work with the Permanence Guarantee. It is this combination of experience and passion that allows our team to provide the best hair removal results, and to keep your skin hair free, forever.
PCOS - the syndrome in detail

As a syndrome with unknown causes PCOS cannot be diagnosed by a simple test. It must be diagnosed by the presence of a collection of symptoms. Since these symptoms can appear unrelated and relatively mild for many years, women can endure them for decades before they are either picked up during tests for other conditions or while being tested for infertility.
History
Symptoms
Menstrual Disorders – either oligomenorrhea (few or irregular periods) or amenorrhea (no periods).
Infertility – resulting directly from the irregular or lack of periods.
High levels of masculinising hormones – elevated levels of testosterone result in hirsutism (male pattern hair growth in a female); acne and oily skin; male pattern baldness and hypermenorrhea (heavy and prolonged periods when they do occur).
Cause
The cause of PCOS is thought to be genetic through a gene inherited from either parent. This leaves a child with a 50% chance of inheriting the disease but gives no indication of how severely the child, if female, will be affected.
In males the same gene may express itself in early onset baldness and excessive hairiness over the rest of the body or the male may remain asymptomatic. The specific gene involved is yet to be identified.
Definition
A woman is defined as having PCOS if any 2 of the following 3 criteria are met and other factors are excluded that would also cause them:
- Few (oligoovulation) or no (anovulation) menstrual periods
- Excess male hormone activity
- Polycystic ovaries

Diagnosis
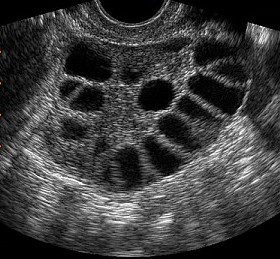
Importantly, not all women with PCOS have polycystic ovaries. A pelvic ultrasound will be used to check for polycystic ovaries but a negative finding does not rule out PCOS.
In a normal menstrual cycle one egg is released from a ripe follicle on the ovary. The follicle then shrinks and disappears within 12 to 14 days. On an ovary affected by excess hormones, several follicles begin to ripen at once but their development is arrested and none reach ovulatory size.
In a pelvic ultrasound, the examiner is looking for a telltale “string of pearls” – a row of 12 to 25 partly ripened follicles to make the diagnosis of polycystic ovaries. It is important to remember that the name polycystic is a little misleading in that there are no actual cysts on the ovaries only that the many (poly) immature follicles (cysts) look like cysts on the surface of the ovaries. A simple blood test is taken to measure levels of hormones such as testosterone. While there are several ways of measuring hormone levels, free-testosterone level is thought to be the most reliable indicator.
Talk to us Today.
Permanence is dedicated to fulfilling your desire for beautiful, hair-free skin. We aim to remove hair once, permanently – and we back the work of our skilled therapists and unique equipment with our Permanence ‘Hair Free for Life’ Guarantee.